
A Quick Overview of the 340B Program
The federal 340B Drug Pricing Program allows qualifying healthcare centers and hospitals (“covered entities”) that serve low-income and uninsured patients to buy prescription drugs at discount rates directly from manufacturers. The intention was to help these providers stretch their limited resources to better serve vulnerable populations.
The program has grown rapidly due to the expansion of covered entities, the increase in contract pharmacies, the introduction of new high-cost therapies, and the rising prices of pharmaceuticals. In 2022 alone, covered entities purchased an estimated $53.7 billion of drugs under the program. Since 2015, the program has grown by an average annual rate of 22.3%.
Overall, the 340B Program has grown to become the second largest drug program behind Medicare Part D. With that many dollars flying around, controversy has followed, from all stakeholders involved, and the program has faced increased scrutiny and criticism in recent years.

History of 340B
The seeds of the 340B program were planted in a drug rebate program contained in the Medicaid Drug Rebate Program (MDRP) created in 1990. But MDRP introduced unintended consequences for safety-net providers. In shifting to this new program, manufacturers halted their existing drug discounts, thus inadvertently increasing costs for safety-net hospitals, Federally Qualified Health Centers (FQHC), and other provider groups serving Medicaid populations that were previously eligible for these discounts. So, because these crucial providers were left out to dry as a result of the MDRP, in 1992, Congress enacted Section 340B of the Public Health Service Act under the Veterans Health Care Act.
Under 340B, in order for drugs to be covered by Medicaid and Medicare Part B, drug manufacturers were now required to pay rebates on outpatient drugs purchased by state Medicaid programs. Those rebates would ensure drug reimbursement for state Medicaid programs at a much lower price point – complying with a “best price” policy – that allowed plans to pay no more than the lowest price paid by any commercial payer.
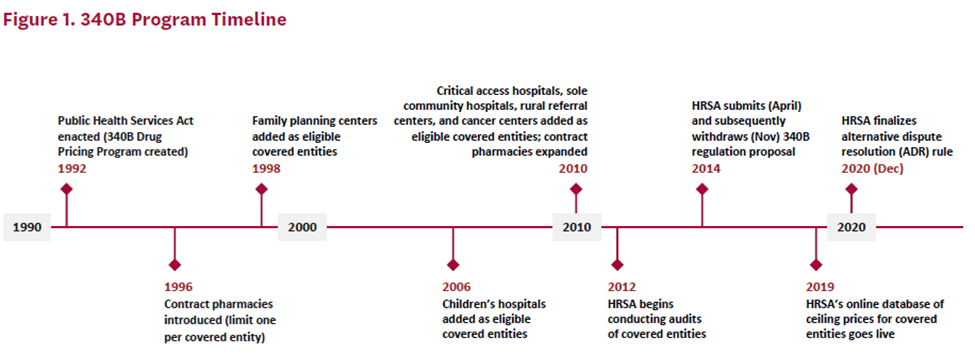
And thus, the 340B Program was born.
Section 340B required drug manufacturers that wish to participate in Medicaid and Medicare Part B to enter into a similar agreement with the federal Department of Health and Human Services (HHS), the agency that runs Medicaid. The agreement requires manufacturers to sell outpatient drugs at discounted rates to eligible “covered entities.” These covered entities include federal Health Resources and Services (HRSA) supported health centers, Ryan White clinics, state AIDS Drug Assistance programs, Medicare/Medicaid Disproportionate Share Hospitals, children’s hospitals, and other safety-net providers.
The 340B program was created with good intentions and made sense at the time. It aimed to help covered entities (mostly safety net providers), generate savings by dispensing discounted drugs, and reinvest the savings into services for the community.
Unfortunately, policymakers failed to understand that no matter how well-meaning the policy, a free market will capitalize on any possible business advantage. “As the 340B program grew, drug manufacturers began looking for ways to reduce their financial exposure,” says Proximity CEO Scott Johnsen. “Spotting a market opportunity, a small group of tech solutions emerged that enabled drug manufacturers to place restrictions on the types and volume of discounts provided to covered entities. Manufacturers leveraged their control over supply to force covered entities to comply or risk losing access to 340B-priced drugs altogether. Following that precedent, an emboldened stakeholder ecosystem began using its own leverage within the operational and financial flows of the program to improve their share of 340B dollars. If you’re a covered entity, this means you’ll need additional resources to manage the growing complexity of a program that is beginning to return less and less value. The result is a loss of financial resources that would have otherwise gone to maintain their capacity to care for patients. For even less fortunate covered entities, it has meant facility closure.”
As you can see, the complexity of this program requires some explanation. Let’s jump into the deep end of how the 340B sausage gets made.
Mechanics of 340B
Below is an example of how the flow of funds could work:
- Step 1 – Setting Prices: The drug manufacturer decides on a price to sell the drug. In this scenario, let’s say it is $120.
- Step 2 – Hospital Purchases Drugs: A 340B-covered entity buys drugs at a discounted price. In our example, the 340B covered entity gets a 50% discount, paying $60 for the drug.
- Step 3 – Dispensing the Drug: Eligible patients get the drug from the covered entity’s pharmacy or a contracted pharmacy which has an agreement with the covered entity to dispense the drug on their behalf.
- Step 4 – Billing Insurance: The provider bills the patient’s insurance for reimbursement. Regardless of whether it’s a 340B hospital or not, the reimbursement amount is the same, which, in this case, would be $120.
- Step 5 – Savings for 340B Hospitals: Because of the discounted purchase price, 340B hospitals save money compared to what they would have paid without the discount. Their net gains from the drug, in this example, would be $60 ($120 – $60) in addition to dispensing fees that they may also get if they are the dispensing pharmacy.
Please note that this is an abstracted view, and the numbers presented here are simplified for the sake of clarity. There are numerous underlying factors and nuances that can significantly influence these figures further.
There are a number of key stipulations to this program which complicate matters. Some have argued that these stipulations lack sufficient clarity and specificity, which has led to many legal disputes. Below are some examples of these stipulations.
First, the discounted prices set by manufacturers may not exceed the 340B ceiling price, which is calculated based on specific formulas outlined in the program regulations. The discount is usually derived from the Average Manufacturer Price (AMP). Presently, the average discount off the drug’s AMP is ~23.19% for brand-name drugs and ~13% for generic drugs. However, the discounts also scale if manufacturers raise prices faster than inflation, resulting in some drugs with very high discount rates.
Second, covered entities are authorized to dispense 340B drugs only to “eligible patients” who have an established relationship with the entity and have received healthcare services from it. To extend their reach and serve populations they might not otherwise access, covered entities often enter into agreements with contract pharmacies, allowing them to dispense 340B drugs to those eligible patients. Those pharmacies purchase drugs at 340B pricing on behalf of the covered entity and dispense them to eligible patients. In this case, the covered entity would profit from the drug discount, and the contract pharmacy would benefit from dispensing fees.
Third, covered entities are prohibited from purchasing a drug at a 340B discount and then submitting a claim to Medicaid for reimbursement, which would result in a rebate being paid to the state Medicaid agency. This is problematic because it can lead to “double rebating”, where both the 340B discount and a separate Medicaid rebate are applied to the same drug, effectively resulting in an unintended overpayment. This situation occurs due to data transparency issues, where the coordination between the 340B program and Medicaid reimbursement processes is not always clear, leading to accidental instances of double rebating.
Evolution of 340B
In 2010, with the passage of the Affordable Care Act (ACA), the eligibility criteria for the 340B program expanded. This expansion significantly broadened the scope of the program, with the number of hospital-covered entities expanding from just 10% to more than 60% by 2021.
Additionally, a policy change implemented by HRSA altered how covered entities can engage with contract pharmacies for filling 340B medications. Previously, covered entities without an in-house pharmacy were restricted to contracting with a single external pharmacy. However, the new policy allows covered entities to contract with an unlimited number of contract pharmacies. This policy shift resulted in a more than 10x increase in contract pharmacies participating in 340B. Today, 340B covered entities have, on average, 20 contract pharmacies in their network. While most providers have 10 or fewer contract pharmacies in their network, select healthcare systems have built extensive contract pharmacy networks.
These policy changes resulted in a significant increase in prescription volume under the 340B program which, in turn, has attracted greater scrutiny.
How 340B Is Shaping Market Opportunities
Given the significance of this program for many stakeholders, we expect to see continued attention and investment in this space. Several areas where we are seeing innovation momentum include:
Specialty Pharmacy Enablement
As margins tighten in other areas of care delivery, providers are turning to in-house specialty pharmacy dispensing to generate additional sources of revenue. The economics of 340B make this especially appealing for providers. Some healthcare systems also view in-sourcing their specialty pharmacy dispensing as a defensive strategy amidst regulatory uncertainties surrounding contract pharmacies and as a way to better control their own fate (i.e., controlling how they optimize 340B capture). Many also argue that medically integrated dispensing (where medical care and the pharmacy are co-located) has been shown to be better for patients. For example, patients can start their treatments sooner and are more likely to stay on them.
Given the complexities of specialty pharmacy, many providers are partnering to stand up their own specialty pharmacy. Shields and Trellis were early entrants that were focused on the health system segment. We are now seeing new players emerge that aim to serve other provider segments. House Rx, for example, provides the technology and services support that enable specialty clinics to dispense medications.
Program Optimization
There is currently a lot of manual work involved in managing and optimizing revenue from the 340B program. This includes pharmacy claims reconciliation and maximization, maximizing referral capture, financial reporting, and audit management. Providers have teams of analysts doing this work. There is plenty of opportunity for providers to employ software to automate aspects of the 340B program operations. This is also an area where AI can create a lot of value.
Reporting & Compliance
We expect to see significant program reform around data reporting. The SUSTAIN 340B Act calls for more information reporting from 340B covered entities to ensure compliance. However, this information may sit on many disparate systems or may not even be tracked.
Discount Reporting
Another prime example of where we see market opportunity concerning 340B is discount reporting. Since the discount is often managed by the contract pharmacy, manufacturers lack provider or patient-level data regarding discount recipients. This lack of transparency raises concerns among manufacturers about potential double rebating, where 340B discounts may be applied when patients are already receiving other price concessions for the same drug. There are opportunities to enhance reporting to provide pharmaceutical companies with insights into how rebates are distributed. Moreover, such reporting would help pharmaceutical companies gain a clearer understanding of prescribing patterns within this patient population.
Proximity is an example of a company addressing a few of these market opportunities, including program optimization, reporting and compliance, and discount reporting. The company is leveraging AI to create automated pharmacy workflows starting with pharmacy claims reconciliation, financial reporting, and audit management as its initial use cases. Proximity continuously integrates and streamlines 340B program data across a covered entity’s network, offering a real-time, comprehensive view of their program, which facilitates revenue capture and compliance monitoring.
Final Thoughts
Driven by innovation and the need for improved care management, the evolution of the 340B program underscores its growing importance in the healthcare landscape. But many are questioning the future of this deeply integrated program: Will it be dismantled? We believe that’s unlikely, as numerous provider groups rely on it for essential revenue. Eliminating the program would shift funding burdens to taxpayers. Instead, we anticipate that the program will continue to evolve, incorporating more regulations to ensure funds are used for their intended purposes.
This presents an opportunity for new entrants to enhance the program’s effectiveness, allowing it to fulfill its mission: “To stretch scarce federal resources as far as possible, reaching more eligible patients, and providing more comprehensive services.”
Sources & Additional Reading
- https://avalere.com/insights/what-is-the-role-of-340b-grantees
- https://www.drugchannels.net/2023/09/exclusive-340b-program-reached-54.html
- https://www.aha.org/guidesreports/2024-03-12-340b-drug-pricing-program
- https://www.drugchannels.net/2023/07/exclusive-for-2023-five-for-profit.html
- https://pioneerinstitute.org/340babuse/growth-of-340b-program/
- https://www.youtube.com/watch?v=0UPOC67WTds
- https://www.youtube.com/watch?v=SpeqIW7ALr8
- https://healthpolicy.usc.edu/research/the-340b-drug-pricing-program-background-ongoing-challenges-and-recent-developments/
- https://www.drugchannels.net/2023/09/exclusive-340b-program-reached-54.html#:~:text=For%202022%2C%20discounted%20purchases%20under,%2452.3%20billion%20(%2B%242.6%20billion)
If you are innovating in this space, or you’d like to discuss this topic with us further, we’d love to talk to you. Please email Josh Flum (jflum@lrvhealth.com) or Lise Courtney D’Amico (lcdamico@lrvhealth.com).




